Untreated Hypertension
Using the PRA test to identify and treat excess sodium or excess PRA
About one in three hypertensive patients has PRA < 0.65 ng/ml/hr. PRA is too low to be a major factor in sustaining the high BP. That patient is likely to respond to a natriuretic (anti-V) drug. (See Anti-V&R drug types under Treatment Guidelines.) Other patients have PRA > 0.65 ng/ml/hr. In them, PRA is helping to sustain the hypertension. These patients are likely to respond to an anti-R drug. They may also respond to an anti-V drug, but the anti-R drug is tested first because PRA is associated with increased cardiovascular risk (1). If BP is not controlled by a full dose of the first drug, PRA is measured again and anti-V or R drugs are added depending on the PRA level.
Visit by visit description
A GENERAL DESCRIPTION OF THE TREATMENT STRATEGY BASED ON V AND R CONCEPTS (REF:2-6)
About 60% of patients can be effectively treated long term with V or R monotherapy.
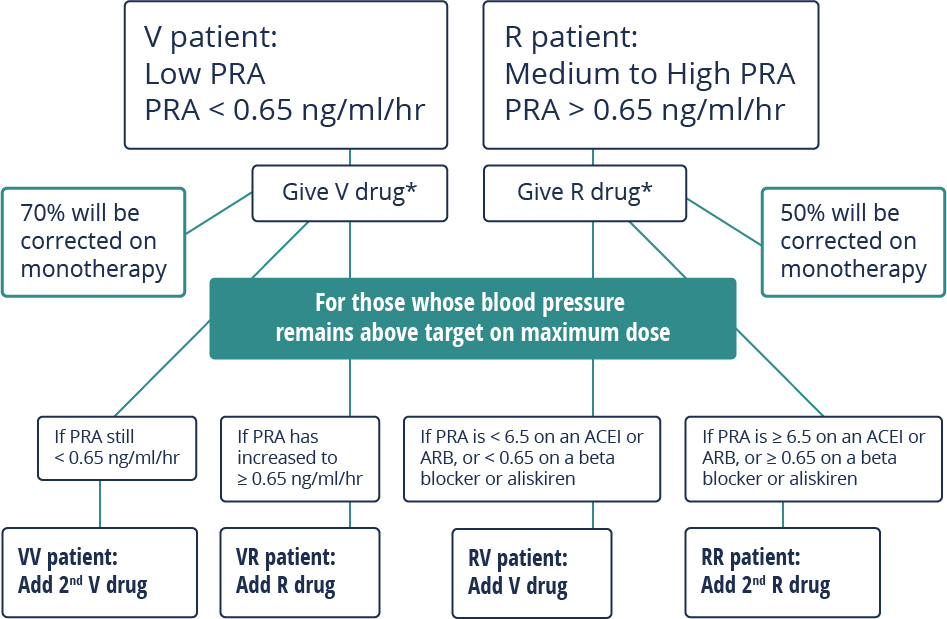
The first step is to find out if the pretreatment ambulatory PRA level is low (PRA < 0.65 ng/ml/hr: V patient) or not low (PRA > 0.65 ng/ml/hr: R patient).
V patients are volume expanded and need to start treatment with a natriuretic V drug (eg spironolactone 12.5 mg/day).
R patients have too much circulating renin and need to start treatment with an anti-renin system R drug (eg enalapril 5 mg/day).
But, the BP of some patients is not fully corrected with full dose monotherapy. A 2nd PRA test can then be used to determine if the reason is because of excess sodium-volume or excess renin.
VV patients are V patients who continue to have low PRA levels while taking a natriuretic drug, indicating that they remain overly volume expanded. They benefit from the addition of a 2nd V drug such as amlodipine (5-10 mg).
VR patients are also V patients, but their on-treatment PRA level increases into the medium range while taking a V drug. They benefit from the addition of an R drug such as enalapril 5 mg to curtail the excess R.
RV patients are R patients whose PRA level while taking an ACEI or ARB remains < 6.5 ng/ml/hr, indicating that PRA has been effectively blocked (ACEIs and ARBs block PRA by about 90%). RV patients are likely to benefit from the addition of a V drug, such as spironolactone 12.5 mg.
RR patients are R patients whose PRA level while taking an ACEI or ARB has increased to > 6.5 ng/ml/hr, indicating that PRA has not been effectively blocked. They are likely to benefit from the addition of a drug that suppresses renin secretion such as a beta blocker like bisoprolol 5 mg.
- Alderman MH, Madhavan S, Ooi WL, Cohen H, Sealey JE, Laragh JH: Association of renin/sodium profile with risk of myocardial infarction in patients with hypertension. N Engl J Med 324: 1098-1104, 1991.
- Laragh J. Laragh’s Lessons in Pathophysiology and Clinical Pearls for Treating Hypertension. Lesson XVI: How to choose the correct drug for each hypertensive patient using a plasma renin-based method and the volume-vasoconstriction analysis. Amer J Hypertens 2001:14:491-503.
- Laragh JH, Sealey JE. The plasma renin test reveals the contribution of body sodium-volume content and renin-angiotensin vasoconstriction to long term blood pressure. Am J Hypertens 2011;24:1164-1180
- Furberg C. Renin test-guided drug treatment of hypertension: The need for clinical trials. Am J Hypertens 2011;24:1158-1163.
- Gharaibeh KA, Turner ST, Hamadah AM, Chapman AB, Cooper-Dehoff RM, Johnson JA, Gums JG, Bailey KR, Schwartz GL.. Comparison of blood pressure control rates among recommended drug selection strategies for initial therapy of hypertension. Am J Hypertens. 2016;29:1186-94.
- Schwartz GL, Bailey K, Chapman AB, Boerwinkle E, Turner ST. The role of plasma renin activity, age, and race in selecting effective initial drug therapy for hypertension. Am J Hypertens. 2013;26:957-964.